 ![]() Dear Social Media Staff At State of California Auditor's Office,
My name is James Martin Driskill. I am not like any other person that you have ever met. I am ANGRY! [😡]. I am justifiablly angry!
To the human person who is reading this now, how can I be personally angry at you? But then again I am!
Because, preconclusively you too will just ignore me like everyone else! For no good reason you will ignore me, even as i have attempted to compell the truth to come forward! For you too must intentionally ignore me, the only deductive reasoning would be that you do not believe in the truth. And that truth must not be told here.
Would that be true? If not, prove it to me. Before you read anything further, respond to all, and say
"Mr Driskill, I have your letter and I have not yet read it. But I promise it will be taken into proper care and concern. Signed: Your Personal Human Name"
But you will not do that. What is it that stops you from doing that?
You will have to CIRCLE THE WAGONS to TREAT ME AS SOME KIND OF THREAT TO YOUR EXISTENCE! BECAUSE I REPRESENT THE TRUTH AND IN THAT TRUTH, IT MUST BE IGNORED FOREVER!
I obviously have no faith that you can do your job properly -- you will fail! Just like everyone else including my very own family! 🔮FAIL 🔮FAIL 🔮FAIL!🔮 That emoji has meaning and purpose.
You will and must fail! This is a text snippit out of a 2003 publication on the National Insitutes of Health -- why is this standard not offered to me? The importance of developing rapport with patients cannot
be overemphasized. Effective communication skills are a critical tool
that assists the physician in establishing that optimal patient rapport.
Physicians need to keep in mind that today's health care consumers,
particularly those in the baby boomer and younger age groups, have much
more medical knowledge than senior citizens. Both young and old,
however, often judge the quality of care received on the basis of the
physician-patient interaction. Certainly, the physician's skill and
reputation play an important role in a patient's confidence. However,
many if not most patients assume that physicians have the requisite
technical skill to treat their medical problems. From the patient's
perspective, therefore, what separates the adequate or average physician
from the truly great physician is how well the physician practices the
“art” of medical care, conveying those highly valued human skills of
compassion and caring concern that patients seem to need so much.
All
too often, when physicians do not communicate caring concern,
especially when the care is painful, difficult, or results in
less-than-optimal outcomes, an inevitable cycle of miscommunication
occurs among patient, family, and physician. Under these circumstances,
patients who express their anger and frustration may cause the physician
to react defensively in a way that may be perceived as hostile or
arrogant. Most often it is this response that causes the patient to seek
the advice of an attorney, because poor communication between a
physician and patient can lead an already angry, dissatisfied patient to
believe the care was poor even when it was entirely appropriate (5). In the arena of physician liability, the burden of “successful” patient-physician communication lies with physicians (5).
That is not to say that patients do not share the burden, but society
and the courts have deemed that physicians have the ultimate
responsibility for initiating, clarifying, facilitating, documenting,
and reinforcing discussions related to their patients' condition,
treatment, and prognosis (5).
i am going to use the FEEDBACK option on the site -- SOMEWHERE, SOMEHOW, SOMEONE is going to STEP FORWARD and START TELLING THE TRUTH! MERCY MERCY MERCY! STOP THE HATE ALREADY!
-----
Stop the lies and stop the hate already!
.png) Why is that not offered to me? From anyone? Anywhere of our civil society?
PLEASE FOLLOW THE DIRECTIONS AS I HAVE PLACED THEM BEFORE YOU,.
THIS SITATION IS OUTRAGEGOUS!
I AM EXPECTING CAPTAIN CARRINGTON TO CONTACT THIS FAMILY TO ARRANGE AND HAVE AN INTERVIEW WITH ME.
ESPECIALLY AS IT RELATES TO THE SUBJECT OF "GANGSTALKING" NOTED BELOW IN MY FULL COPY OF MY MENTAL HEALTH CARE
RECORD THAT WAS VERY VERY VERY VERY TARDY ONLINE,.
COMPLETLY BLANK MEDICAL RECORDS -- SERIOUSLY BLANK! http://awesomekramoboneplayroom.school/TechnoREALism/
MEME 4.02 In this issue of MEME: TECHNOREALISM Over the past few months, I participated in the creation of a set of principles called "technorealism." It's a set of declarations meant to go beyond the bi-polar visions of cyber-utopianism and neo-Luddism. In another age, this would be considered a manifesto. Now it is an open letter, a document which, through the Internet, takes on a fluid, dynamic form. Literally anyone can sign it, pass it on, and participate. Instructions on how to do this appear at the end of this message. If you like what you read, I urge you to forward it, to friends, colleagues, and other lists where appropriate. Without further delay, let me introduce you to Technorealism. David S. Bennahum, New York City, March 11, 1998. http://memex.org/meme4-02.html
---- TECHNOREALISM
PRINCIPLES OF TECHNOREALISM 1. Technologies are not neutral.
A great misconception of our time is the idea that technologies are completely free of bias -- that because they are inanimate artifacts, they don't promote certain kinds of behaviors over others. In truth, technologies come loaded with both intended and unintended social, political, and economic leanings. Every tool provides its users with a particular manner of seeing the world and specific ways of interacting with others. It is important for each of us to consider the biases of various technologies and to seek out those that reflect our values and aspirations. 2. The Internet is revolutionary, but not Utopian.
The Net is an extraordinary communications tool that provides a range of new opportunities for people, communities, businesses, and government. Yet as cyberspace becomes more populated, it increasingly resembles society at large, in all its complexity. For every empowering or enlightening aspect of the wired life, there will also be dimensions that are malicious, perverse, or rather ordinary. 3. Government has an important role to play on the electronic frontier.
Contrary to some claims, cyberspace is not formally a place or jurisdiction separate from Earth. While governments should respect the rules and customs that have arisen in cyberspace, and should not stifle this new world with inefficient regulation or censorship, it is foolish to say that the public has no sovereignty over what an errant citizen or fraudulent corporation does online. As the representative of the people and the guardian of democratic values, the state has the right and responsibility to help integrate cyberspace and conventional society. Technology standards and privacy issues, for example, are too important to be entrusted to the marketplace alone. Competing software firms have little interest in preserving the open standards that are essential to a fully functioning interactive network. Markets encourage innovation, but they do not necessarily insure the public interest. 4. Information is not knowledge.
All around us, information is moving faster and becoming cheaper to acquire, and the benefits are manifest. That said, the proliferation of data is also a serious challenge, requiring new measures of human discipline and skepticism. We must not confuse the thrill of acquiring or distributing information quickly with the more daunting task of converting it into knowledge and wisdom. Regardless of how advanced our computers become, we should never use them as a substitute for our own basic cognitive skills of awareness, perception, reasoning, and judgment. 5. Wiring the schools will not save them.
The problems with America's public schools -- disparate funding, social promotion, bloated class size, crumbling infrastructure, lack of standards -- have almost nothing to do with technology. Consequently, no amount of technology will lead to the educational revolution prophesied by President Clinton and others. The art of teaching cannot be replicated by computers, the Net, or by "distance learning." These tools can, of course, augment an already high-quality educational experience. But to rely on them as any sort of panacea would be a costly mistake. 6. Information wants to be protected.
It's true that cyberspace and other recent developments are challenging our copyright laws and frameworks for protecting intellectual property. The answer, though, is not to scrap existing statutes and principles. Instead, we must update old laws and interpretations so that information receives roughly the same protection it did in the context of old media. The goal is the same: to give authors sufficient control over their work so that they have an incentive to create, while maintaining the right of the public to make fair use of that information. In neither context does information want "to be free." Rather, it needs to be protected. 7. The public owns the airwaves; the public should benefit from their use.
The recent digital spectrum giveaway to broadcasters underscores the corrupt and inefficient misuse of public resources in the arena of technology. The citizenry should benefit and profit from the use of public frequencies, and should retain a portion of the spectrum for educational, cultural, and public access uses. We should demand more for private use of public property. 8. Understanding technology should be an essential component of global citizenship.
In a world driven by the flow of information, the interfaces -- and the underlying code -- that make information visible are becoming enormously powerful social forces. Understanding their strengths and limitations, and even participating in the creation of better tools, should be an important part of being an involved citizen. These tools affect our lives as much as laws do, and we should subject them to a similar democratic scrutiny. ------
Enough is Enough -- No More Lies - Don't Lie To me! ![[DIR]](./Gmail - Fwd Family Matters Really This family sucks!_files/unnamed(8).gif) Honesty/ 2020-10-06 20:31 Honesty/ 2020-10-06 20:31
Plays YouTube Music Honesty By Billy Joel
Plays YouTube Playlist Starting With Barbra Streisand - Don't Lie To me!
Here is that playlist:
Time To Gruwup From The World Of Lies Cheats and Stealing Our Collective PeaceMakta Pond
1 / 16
4:02
Barbra Streisand - Don't Lie to Me (Official Video)
Barbra Streisand
4:49
Donna Summer - No More Tears (Enough Is Enough) (Duet With Barbra Streisand)
ALPHA BETA
3:24
VERY LEGAL AND OUT OF THE BOX METHOD - dbh.sbcounty.gov - Dr. Veronica Kelley Director
James Driskill
9:06
Corrupt Police Gangs Wreak Havoc In Chicago
The Young Turks
2:13:45
Absolutely WALLED OUT Access To Care -- Intentional Harm Done Here - #BigManKillingTechBug
Makta Pond
9:53
The Community As A Whole Must Seek To Understand Each Other! [#09]
Makta Pond
7:59
Heart - Stairway to Heaven (Live at Kennedy Center Honors) [FULL VERSION]
Don Jack
15:06
How to build (and rebuild) trust | Frances Frei
TED
2:11:39
Being Myself Is Not More Than Enough I Want to Die! No Help From Any Source I Reach To!
Makta Pond
37:59
Overcoming Addiction - The Root Cause Of Every Addiction
Actualized.org
1:50:46
Gua Gua Gua Guilty Guilty Dah - San Bernardino Police Dept - Lt. Nelson Carrington - Fail Fail Fail
Makta Pond
20:41
Watch All In With Chris Hayes Highlights: August 5th | MSNBC
MSNBC
23:10
FTP Transfer Held @FuckedUpHuman.Net Memespace Blown Up Filenames Passersby Real People Wrecked Feet
Makta Pond
4:35
How do you know whom to trust? - Ram Neta
TED-Ed
10:57
The First Impression Hoax | Charlene Rocha | TEDxStMaryCSSchool
TEDx Talks
22:58
Why trust is so important and how we can get more of it? | Dan Ariely | TEDxJaffa
TEDx Talks
I am going to use FEEDBACK
Stalking by individuals has been found to result in high rates both of psychological distress and lasting psychiatric morbidity, in particular post-traumatic symptomatology and depression [1,4,10,18,19,20]. The one study to examine the psychological sequelae of the experience of being gang stalked found that individuals who had been group or gang stalked scored significantly higher on ratings of depressive symptoms, post-traumatic symptomatology and adverse impact on social and occupational functioning than those who were individually stalked [5]. The only other published study of gang-stalking samples that we could locate detailed four cases reported by the media of men who had engaged in extreme violence as a response to the perception that they were the target of gang stalkers [21]. Both Sheridan and James [5] and Sarteschi [21] concluded that the subjects of their studies were suffering or had suffered from severe psychological distress in the context of their subjective gang-stalking experiences.
A VERY SICK FAMILY! DEVOID OF ITS SENSES! THIS QR SCAN CODE ACCESS THIS EMAIL THREAD UPDATES AS NECESSARY.
WE SHOULD NOT BE IN THE SITUATION WE ARE IN
THIS FAMILY HAS BETRAYED ME!
QR CODE URL:
REFERENCE:
SO WHAT IF I AM LOUD?
SO WHAT IF I AM A BIT OF CRAZY?
THERE IS NO LOVE HERE FOR SURE!
THIS ALREADY HAS BEEN PLACED ONLINE -- YOU ALL ARE HURTFUL AND HATEFUL TOWARD ME! THAT IS A FACT!
OBVIOUSLY, THIS HERE DOES NOT EXIST UNDER THIS ROOF:
SABOTAGE MY EFFORT TO GET A PROPER DOCTOR\ RELATIONSHIP IN HIV CARE SINCE DOCTOR SHIGENO DID THIS TO ME!
QR CODE:
WHAT HAPPENED WITH DOCTOR BASSI?
WE CAN'T TALK ABOUT THAT IN THE NEW DOCTOR RELATIONSHIP? NOT BEING SWEPT UNDER THE RUG!
QR CODE:
TUFF SPOTS?
THIS IS FATAL!
This is a RECORD of TRANSMISSION of a FAX that WAS CONFIRMED -- but the
action by the DOCTOR does not RELATE processing. The fax is about the
initiation of PATIENT-CENTERED communications. It does not make any
sense that I can not assert these needs into my care with my HIV
Disease. This matter must be put upward into a counsel of higher
authority -- The Federal Bureau of Investigation - and joined to be
UNITED FORCE to call downward reprimands upon the wrong way of thinking and
insane blocking PATIENT-CENTERED REQUIRED BY LAW to BE PRESENT and
ACCOUNTED FOR -- ENFORCED LAW MEDICAL CARE INTERFACES!
So far, a story of great tragedy!
Attention General Public
Visitors To This Page, this is not a very fun thing to read. I suggest
if you are looking for just a distraction in blimp of time. This page is
not for you.... but you are free to find the reasons why you were
directed to this page. Thank You.
Without Doctor Care In HIV
Corrected Adaptive To The Conditions That Are In This Address -- You are
Guilty of a Conspiracy So Vast -- I will DIE First before you are
allowed to be SILENT to these circumstances -- not one doctor will do
their jobs professionally -- in this conspiracy - I am being restricted
from medical care for a need to maintain a secretive agenda mentioned in
this holding note -- I will DIE in pain than to allow you to get away
from this madness! I should have medical care privacy, but I can't
because of this shit!

PRETTY? UGLY? No TRUSTWORTHY DOCTOR is willing to SET THEM SELF into
INTEGRITY! I WILL DIE FIRST THAN TO COMPROMISE TO RECEIVE THE CARE OF
ANY DOCTOR WHO CAN NOT BECOME HONEST WITH THIS ISSUE -- FUCK YOU ALL
HATERS!
YOU SAY, MAMA, "TIME IS RUNNING OUT"
COMMIT TO THE TRUTH!
I AM DONE WITH YOUR ALL GAMES.... WITHOUT A FAMILY SUPPORTIVE
TRUE INTERVENTION TO SHOW YOURSELVES IN FULL SUPPORT OF MY NEEDS
GO TO HELL! THEY ARE INDEED TRYING AND WILL SUCCEED IN MURDERING ME!
.png) Kareo Patient Portal Kareo Patient PortalInland Psychiatric Medical Group Portal Messaging To Doctor JAGAN MOHAN RAO JAKKULA Saturday May 14th 2022 4:48 PM
Subject: [ Keeping it Real ] -- There is an emoji for this [ 💯]
Message: The meaning of that emoji is a SCORE of 100% or of EXCELLENCE!
I had not logged in for a while to Inland Psyche / Patient Portal because none of my records were updated and the interactions with my doctors are as I have said they are. I am the patient and the patient has had something to say profoundly to the criticism of what has been the operating agenda of this entire equation seems way offensive off the mark offensive.
I write about it online and have given it a tag [ #BigManKillingTechBug ]
I do not accept that you all just turn around [ for me ] and that turnaround does not apply to real true grit policy and change in your organization. I do not accept an underhanded change that now puts items into my medical record. Especially considering I have not even checked it for errors and/or omissions. I NEED TO HAVE A DETAILED LOG OF WHEN THE DETAIL WAS UPDATED TO MY RECORDS!
WITHOUT DECEPTION! This whole thing has shattered my family relations!
------ MEDICAL RECORD SEARCH
YES, DOCTORS, THIS IS BEING PLACED PUBLIC -- I HAVE NO OTHER CHOICE
BECAUSE YOU FAIL TO CONCEDE TO AN AUDIT PROPERLY!
THIS IS A REALITY AUDIT! I HAVE ABSOLUTELY NOTHING TO HIDE!
THEY KNOW AS WELL AS I DO THAT THESE FIELDS HAVE VALUES THAT I SUBMITTED IN DETAIL! AND A COPY OF THAT IN MY OWN FILES!
NOTE:
SEE THE VERY LAST COMMENTING SECTION OF THIS EMAIL Kareo Patient PortalMessages[ Keeping it Real ] -- There is an emoji for this [ 💯 ]James Driskillto JAGAN MOHAN RAO JAKKULA5/14/22 4:47 PM
------------
Inland Psychiatric Medical Group
|
DRISKILL
, JAMES
|
|
|
74455486755769533301390734623137025694
MRN
|
|
|
|
3260 Grande Vista
San Bernardino, CA 924051939
Address
|
|
Not Hispanic or Latino
Ethnicity
|
|
-
instructions
-
medical devices
-
procedures
-
encounters
-
problems
-
Treatment Plans
-
Immunizations
-
health concerns
-
goals
-
mental/functional status
-
chief complaint
-
assessments
-
reason for referral
-
social history
-
medications
-
vital signs
-
insurance providers
-
family history
-
results
-
Allergies
-
clinical notes
medical devices
| GMDN Name |
UDI |
Expiration Date |
Status |
| No Information Available |
procedures
| Name |
Related To |
Notes |
Date |
| No Information Available |
encounters
| Encounter |
Performer |
Date |
| Encounter Visit |
JAGAN JAKKULA |
03/07/2022 |
| Encounter Visit |
Yvette Arroyo |
01/31/2022 |
| Encounter Visit |
Breanna Yang |
12/23/2021 |
| Encounter Visit |
Emmy Reyes |
01/20/2022 |
| Encounter Visit |
raviteja ethalapaka |
01/31/2022 |
| Encounter Visit |
Breanna Yang |
03/14/2022 |
| Encounter Visit |
Adrianna Sandoval |
01/20/2022 |
| Encounter Visit |
Olivia Ellis |
01/21/2022 |
| Encounter Visit |
Allyce Turturica |
02/08/2022 |
| Encounter Visit |
SUDHEER JALAGADUGULA |
12/03/2021 |
| Encounter Visit |
VANAJAKSHI GOKAPAI |
01/05/2022 |
| Encounter Visit |
Amber Morris |
01/31/2022 |
| Encounter Visit |
Breanna Yang |
03/08/2022 |
| Encounter Visit |
Julitza Reyes |
05/07/2022 |
| Encounter Visit |
Ashley Welty |
01/31/2022 |
| Encounter Visit |
raviteja ethalapaka |
01/20/2022 |
| Encounter Visit |
Olivia Ellis |
01/17/2022 |
| Encounter Visit |
Wilson Thammavongsa |
03/22/2022 |
| Encounter Visit |
Estefania Landin |
01/07/2022 |
| Encounter Visit |
JAGAN JAKKULA |
03/24/2022 |
| Encounter Visit |
Candelaria Perez |
02/21/2022 |
| Encounter Visit |
Estefania Landin |
12/22/2021 |
| Encounter Visit |
MUBASHIR FAROOQI |
01/06/2020 |
| Encounter Visit |
CHINYERE OBAKHUME |
01/04/2022 |
| Encounter Visit |
Olivia Ellis |
01/31/2022 |
| Encounter Visit |
Estefania Landin |
01/31/2022 |
| Encounter Visit |
Alfonso Cordova |
02/02/2022 |
| Encounter Visit |
PRATHAP THATHAPUDI |
12/02/2021 |
| Encounter Visit |
Estefania Landin |
01/21/2022 |
| Encounter Visit |
Olivia Ellis |
12/28/2021 |
| Encounter Visit |
Breanna Yang |
12/23/2021 |
| Encounter Visit |
Olivia Ellis |
01/20/2022 |
| Encounter Visit |
Jayasree Adireddy |
02/22/2022 |
| Encounter Visit |
Estefania Landin |
01/28/2022 |
| Encounter Visit |
Breanna Yang |
12/22/2021 |
| Encounter Visit |
Amber Morris |
02/04/2022 |
| Encounter Visit |
Ashley Valdez |
03/07/2022 |
| Encounter Visit |
PAVANI KOTHAPALLI |
04/26/2021 |
| Encounter Visit |
Marie Garcia |
04/20/2021 |
| Encounter Visit |
Valerie Perez |
02/28/2020 |
| Encounter Visit |
Ashley Welty |
04/28/2022 |
| Encounter Visit |
Ashley Valdez |
03/05/2022 |
| Encounter Visit |
Estefania Landin |
01/19/2022 |
| Encounter Visit |
Estefania Landin |
02/01/2022 |
| Encounter Visit |
Yvette Arroyo |
02/02/2022 |
| Encounter Visit |
Devin Fallis |
02/19/2022 |
| Encounter Visit |
Emmy Reyes |
01/25/2022 |
| Encounter Visit |
Guadalupe Martin |
01/28/2022 |
| Encounter Visit |
Diane Barrera |
01/31/2022 |
| Encounter Visit |
Estefania Landin |
01/26/2022 |
| Encounter Visit |
zulekha mohammed |
02/02/2022 |
| Encounter Visit |
Breanna Yang |
02/03/2022 |
| Encounter Visit |
Connie Gomar |
04/20/2022 |
problems
| Problem |
Effective Dates |
Problem Status |
| Severe mood disorder with psychotic features (disorder), [26516009] |
20200106 |
ACTIVE |
| Schizoaffective disorder, bipolar type (disorder), [38368003] |
20200106 |
ACTIVE |
Immunizations
| Vaccine Name |
Date |
Status |
|
No Information Available
|
|
|
health concerns
| Health Concerns |
| No Information Available |
goals
| Goals |
| No Information Available |
mental/functional status
| Mental/Functional Findings |
| No Information Available |
chief complaint
| Reason for Visit/Chief Complaint |
| No Information Available |
assessments
| ASSESSMENTS |
pt and mom reports improvement in mood/psychotic symptoms but not
optimally controlled . d/w consider alternate medications , optimize
medication dose -agreeable with plan
will get medical records for review
|
Severe mood disorder with psychotic features (disorder)
(F31.64/296.64) Bipolar disorder, current episode mixed, severe, with
psychotic features modified 6 Jan, 2020
Schizoaffective disorder, bipolar type (disorder) (F25.0/295.70) Schizoaffective disorder, bipolar type modified 6 Jan, 2020
|
pt and mom reports mood/psychotic symptoms not optimally controlled
-off psychotorpics - contributing factors as above. d/w consider
alternate medications , optimize medication dose -agreeable with plan
will get medical records for review from dr farooqi .
|
Severe mood disorder with psychotic features (disorder)
(F31.64/296.64) Bipolar disorder, current episode mixed, severe, with
psychotic features modified 6 Jan, 2020
|
reason for referral
| Reason For Referral |
| No Information Available |
social history
| Social History Element |
Description |
Effective Dates |
| Birth Gender |
Male |
01/04/2022 |
| Smoking Status |
Never smoker, [SNOMED-CT:266919005], null |
2022 |
medications
| Medication |
Start Date |
Instructions |
Status |
|
lamoTRIgine 200 mg tablet, [RxNorm: 198429]
|
01/04/2022 |
1 tab(s) orally 2 times a day
|
Discontinued |
|
LaMICtal 25 mg tablet, [RxNorm: 105019]
|
03/07/2022 |
take 1 tablet daily for 2 weeks then 1 tablet twice a day
|
Discontinued |
|
LaMICtal 25 mg tablet, [RxNorm: 105019]
|
03/24/2022 |
take 2 tablets twice a day
|
active |
|
cariprazine 6 mg capsule, [RxNorm: 1667678]
|
01/04/2022 |
1 cap(s) orally at every bedtime
|
Discontinued |
vital signs
| Date / Time: |
01/04/2022 |
| Height |
172.72 cm
|
| Weight |
83.56 kg
|
| BMI |
28.01 kg/m2
|
| Blood Pressure |
mm[Hg]
|
| Heart Rate |
/min
|
| O2 Percentage BldC Oximetry |
%
|
| Inhaled Oxygen Concentration |
%
|
| Body Temperature |
Cel
|
| Respiratory Rate |
/min
|
| Head circumference |
0 percentile
|
| Weight-for-length |
0 percentile
|
family history
| FAMILY HISTORY |
Family member |
Diagnosis |
|
No Information Available
|
|
|
results
| Name |
Actual Result |
Date |
Laboratory |
|
No Information Available
|
|
|
|
Allergies
| Type |
Substance |
Reaction |
Severity |
Status |
| No Information Available |
|
|
|
|
clinical notes
| CLINICAL NOTES |
CC: NO CURES AVAILABLE 3/5/2022 Requested Dr.P to discuss history with Dr. Jakkula before appointment. Deepa 03/01/2022
As telehealth/video provider, I Jagan Jakkula MD, attest that I
introduced myself to patient, provide the credentials, disclosed my
location , other participants in the virtual visit , and the reason for
real time two way interactive audio and video consult , I and patient
have mutually agreed that this visit is appropriate for video technology
.
Originating site (Patient location) : patients home
Distant location(provider location) : Irvine, California
Psych Syndromes:
Patient seen for follow up for medication management .
accompanied by mom. says he is doing better, says taking lamictal ,just
started higher dose- says tolerating it , says seems to help to some
extent . says still feeling down, anxious somedays . denies panic
attacks .. gets 6-7 hrs sleep/night . noted to be delusional -seems to
be chronic in nature . says he has bipolar -unable to give a clear hx
for manic/hypomanic symptoms . denies command , visual, auditory
hallucinations , suicidal thoughts , self injurious behaviors ,
homicidal thoughts .. reports compliance with medications, tolerating
except as above
substance abuse hx: per chart review- unable get from pt at this time
SUBSTANCE ASSESSMENT HX:
-cannabis: Endorsed
last used last month
-alcohol: denied
-meth/cocaine: endorsed
onset: age 20
amount: < 1 gm/month
last used: a month ago
-Nicotine use/Vaping: never smoke, per patient
Review of systems :
Constitutional: negative
Endocrinology: negative
Skin: negative
Respiratory: negative
Gastrointestinal: negative
Genitourinary: negative
Musculoskeletal: negative
Neurological: negative
psychiatry : see HPI
Medications: Lamictal, take 2 tablets twice a day (Edited by JAGAN JAKKULA on Mar 24, 2022)
MSE:
The patient's speech was normal, sharing conversation with normal
laryngeal efforts. Appropriate mood and affect were seen :better ,
anxious, irritable -mood congruent .. Thought processes -tengential,
disoragnised . dneies suicidal/homicidal thoughts . The patient's
judgement -seems impaired . Mental status included: correct time, place,
person orientation, normal recent and remote memory, normal attention
span and concentration ability. Language skills included the ability to
correctly name objects. Fund of knowledge included normal awareness of
current and past events
DSM-5: Schizoaffective bipolar by hx
Assessment:
pt and mom reports improvement in mood/psychotic symptoms but not
optimally controlled . d/w consider alternate medications , optimize
medication dose -agreeable with plan
will get medical records for review
Plan:
Increase lamictal to 50 mg bid after 2 weeks . psychoeducation
provided about diagnosis ,treatment plan, interactions with other
medications . medication side effects, risks, benefits and alternatives
was discussed including periodic monitoring of parameters
individual therapy recommended
if worsening symptoms , call my office
obtain medical records from previous provider
safety plan:
patient agrees to utilize the following resources in the event of
acute suicidal urges: ER,walk in clinic, crisis line/team, stay with family, structured plans, call contact person
short term goal: obtain all medical records, medication tolerance
long term plan: remission of symptoms and maintain stability
patient understands and agrees with plan
f/u in 3-4 weeks or sooner if needed
|
CC: Requested Dr.P to discuss history with Dr. Jakkula before appointment. Deepa 03/01/2022
As telehealth/video provider, I Jagan Jakkula MD, attest that I
introduced myself to patient, provide the credentials, disclosed my
location , other participants in the virtual visit , and the reason for
real time two way interactive audio and video consult , I and patient
have mutually agreed that this visit is appropriate for video technology
.
Originating site (Patient location) : patients home
Distant location(provider location) : Irvine, California
HPI:
Patient seen for initial evaluation , referred for medication
management . per chart review- patient currently on lamictal,
cariprazine-says he is not taking them , says he is waiting to see this
provider before start taking -says cariprazine is expensive , cannot
afford , wants to try alternate medications . says he has seen dr frooqi
in the past, seen np recently . accompanied by mom. says currently
living with mom . says he needs to get back on his medication . says he
wants this provider to acknowledge "gang stalking" and wants the
provider to read up on "gang stalking" and attest that the disorder
called "gang stalking" is real . says he has been off his medications
for last year . says diagnosed with schizoaffective - bipolar . says
he moved to california since 2017 , says he was diagnosed with bipolar
about 15 years ago. says he was admitted to in pt psych unit few
times-says thinks he was manic at that time . denies hallucinations
.says sleeping ok. says he is very anxious , says he is unable to get
care for his medication . says he is feeling depressed and anxious .
patient endorses low mood, anhedonia ,low energy ,motivation,
hopelessness, , low psychomotor activity, constant racing thoughts ,
unable to relax, fidgety . denies panic attacks . says he is sleeping
well . gets 7-8 hrs sleep/night . noted to be delusional -seems to be
chronic in nature . says he has bipolar -unable to give a clear hx for
manic/hypomanic symptoms -says bipolar gets worse when off medications .
denies ptsd symptoms including nightmares, flashbacks, avoidance .
denies command , visual, auditory hallucinations , suicidal thoughts ,
self injurious behaviors , homicidal thoughts . denies OCD symptoms .
denies childhood hx of ADHD. reports currently off psychotorpics .
substance abuse hx: per chart review- unable get from pt at this time
SUBSTANCE ASSESSMENT HX:
-cannabis: Endorsed
last used last month
-alcohol: denied
-meth/cocaine: endorsed
onset: age 20
amount: < 1 gm/month
last used: a month ago
-Nicotine use/Vaping: never smoke, per patient
Review of systems :
Constitutional: negative
Endocrinology: negative
Skin: negative
Respiratory: negative
Gastrointestinal: negative
Genitourinary: negative
Musculoskeletal: negative
Neurological: negative
psychiatry : see HPI
PsychHx: Reported multiple inpatient psychiatric
holds/hospitalizations: Pennsylvania, in 2017, on his way to Washington
DC, to discuss the topic of "Gang stalking" with authorities; San
Bernardino Comm. Hosp. in 2020; January/2021 - 2 weeks at Arrowhead BMC,
Colton, CA; and October/2021 at Canyon Creek Beh. Health, Texas, for 2
weeks.
RISK ASSESSMENT:
-Suicidal thoughts: patient denied
-History Suicidal Plan/Attempts: patient denied
-Homicidal Ideation: patient denied
-History of Harm to Others: patient denied
-Access to firearms or other weapon(s): mother endorsed, but locked
PMHx: Hyperlipidemia
Type II DM
HIV POSITIVE
PSHx: denies past surgical history
PsychFHx: denies
PsychSHx:
PsychSHx
-Marital Status/Kids: single with no kids
-Living Situation: living with mom, since 2017
-History of Abuse/Traumas: denied
-Employment/School /Occupational Status: on disability benefits
-Highest Education: 12th grade
-Current or Prior Military Service: denied
-Support/Social Systems/Network: mother and friend (Luis)
-Legal/Forensics Hx: jailed once in Texas
-Religion/Spiritual Belief: Christian
-Sexual Preference: identifies as gay
-Use of Herbal/Nutritional Supplements: denied
Medications: Lamictal, take 1 tablet daily for 2 weeks, then 1 tablet twice a day (Edited by JAGAN JAKKULA on Mar 7, 2022)
MSE:
The patient's speech was normal, sharing conversation with normal
laryngeal efforts. Appropriate mood and affect were seen : anxious,
irritable ,sad -mood congruent .. Thought processes -tengential,
disoragnised . dneies suicidal/homicidal thoughts . The patient's
judgement -seems impaired . Mental status included: correct time, place,
person orientation, normal recent and remote memory, normal attention
span and concentration ability. Language skills included the ability to
correctly name objects. Fund of knowledge included normal awareness of
current and past events.
DSM-5: Schizoaffective bipolar by hx
Assessment:
pt and mom reports mood/psychotic symptoms not optimally
controlled -off psychotorpics - contributing factors as above. d/w
consider alternate medications , optimize medication dose -agreeable
with plan
will get medical records for review from dr farooqi .
Plan:
start lamictal 25 mg daily for 2 weeks, then 25 mg bid .
psychoeducation provided about diagnosis ,treatment plan, interactions
with other medications . medication side effects, risks, benefits and
alternatives was discussed including periodic monitoring of parameters
individual therapy recommended
if worsening symptoms , call my office
obtain medical records from previous provider
safety plan:
patient agrees to utilize the following resources in the event of
acute suicidal urges: ER,walk in clinic, crisis line/team, stay with family, structured plans, call contact person
short term goal: obtain all medical records, medication tolerance
long term plan: remission of symptoms and maintain stability
patient understands and agrees with plan
f/u in 3-4 weeks or sooner if needed
|
CC: "I am a targeted individual for 16 years by number of individuals, "
HPI:
A 56y/o, Caucasian, male, seen for initial evaluation, in company of mother (Veronica Driskill)
Seeking services today for management of "gang stalking" and requesting
to know how this provider to treat for "gang stalking" and wants the
provider to read up on "gang stalking" and attest that the disorder
called "gang stalking" is real or he would not proceed with the session.
This provider promised to research the said disorder and will be
informed enough to discuss it at the next session. Patient became
irate, and most of the interval history obtained from his mother.
Patient is known to this practice, with diagnoses of schizoaffective and
depressive disorders. Patient reported of being stalked/followed and
earmarked for destruction. Stated that the stalking drove out of Denver
where he had a home onto street and now living with his since 2017.
Reported multiple inpatient psychiatric holds/hospitalizations:
Pennsylvania, in 2017, on his way to Washington DC, to discuss the topic
of "Gang stalking" with authorities; San Bernardino Comm. Hosp. in
2020; January/2021 - 2 weeks at Arrowhead BMC, Colton, CA; and
October/2021 at Canyon Creek Beh. Health, Texas, for 2 weeks.
He identified as a gay man. Patient suicidal thoughts, auditory/visual hallucinations during the session
-history of cardiac issues/events: patient denied
-history of head trauma: patient denied
-history of seizures: patient denied
-history of chronic pain syndrome: patient denied
DSM-5:
Review of current DSM-V Symptoms:
Depressive symptoms M/B:
+Depressed mood/sadness
+Anhedonia/Motivation
+Feelings of worthlessness/hopelessness
-Excessive guilty
-Sleep disturbance
-Appetite with weight gain/loss
+Poor concentration/attention
Anxiety/Panic Symptoms M/B:
+Anxiety
+Excessive worries
+Difficulty to control, inability shot down one?s mind
-Easily fatigued
+Difficulty concentrating
+Easily irritability
-Sleep disturbance
-Headache and/or muscle tension
-Eyed up or on edge
Mania Symptoms M/B:
Elevated/expansive mood
Racing thoughts
+Distractibility/impulsivity
+Increased in goal-directed activities
-Decreased need for sleep lasting over 24 hours
+Pressured speech
+Grandiose delusions
-Decreased appetite
+Recent Hospitalization
Psychotic Symptoms:
+Delusions
-Hallucinations
+Disorganized speech
+Disorganized behaviors
+Paranoia
+Negative symptoms
ADHD Symptoms:
Inattention Sx M/B:
patient denied
Hyperactive/impulsivity Sx M/B:
patient denied
PSTD Symptoms M/B:
patient denied
OCD SYMPTOMS M/B:
patient denied
EATING DISORDER SYMPTOMS:
patient denied
PsychHx:
SUBSTANCE ASSESSMENT HX:
-cannabis: Endorsed
last used last month
-alcohol: denied
-meth/cocaine: endorsed
onset: age 20
amount: < 1 gm/month
last used: a month ago
-Nicotine use/Vaping: never smoke, per patient
RISK ASSESSMENT:
-Suicidal thoughts: patient denied
-History Suicidal Plan/Attempts: patient denied
-Homicidal Ideation: patient denied
-History of Harm to Others: patient denied
-Access to firearms or other weapon(s): mother endorsed, but locked
PsychSHx: -Marital Status/Kids: single with no kids
-Living Situation: living with mom, since 2017
-History of Abuse/Traumas: denied
-Employment/School /Occupational Status: on disability benefits
-Highest Education: 12th grade
-Current or Prior Military Service: denied
-Support/Social Systems/Network: mother and friend (Luis)
-Legal/Forensics Hx: jailed once in Texas
-Religion/Spiritual Belief: Christian
-Sexual Preference: identifies as gay
-Use of Herbal/Nutritional Supplements: denied
Soc Hx: Tobacco: Never smoker -
Alcohol: Do not drink -
Drug Abuse: Illicit drug use -
Cardiovascular: Eat healthy meals -
Safety: Household Smoke detector -
Sexual Activity: Homosexual encounters - per patient "I am gay"
Birth Gender: Male -
Custom Items: Cannabis -
PsychFHx: mother denied
ROS: Eyes: WNL
Ears: WNL
Nose: WNL
Mouth/Throat/Voice: WNL
Neck: WNL
Respiratory: WNL
Cardiovascular: WNL
Gastrointestinal: WNL
Musculoskeletal: WNL
Neurological: (+) difficulty concentrating
Psychiatric: (+) change in mood, (+)depression, (+)sadness interfering
with function, (+)anxiety, (+)nervousness, (-)sleep disturbance,
(-)suicidal ideation, (+)hopelessness, (+)worthlessness,
(-)hallucinations
has a history of HIV
PMHx: Hyperlipidemia
Type II DM
HIV POSITIVE
PSHx: denies past surgical history
Medications: cariprazine, 1 cap(s) orally at every bedtime (Edited by CHINYERE OBAKHUME on Jan 4, 2022)
lamotrigine, 1 tab(s) orally 2 times a day (Edited by CHINYERE OBAKHUME on Jan 4, 2022)
Allergies: No allergy history has been documented for this patient.
No known medication allergies
MSE: General Appearance/Build: Appeared the stated age of an average built
Grooming/Hygiene: average
Eye contact/Demeanor: erratic
Motor Activity: agitated
Speech: pressured and excessive (dominated the session with irrelevant details)
Mood & Affect: irritable & angry (mood & affect congruent)
Thought Process Disturbances: loose association
Thought Content Disturbances: paranoia "all his discussions were centered on gang stalking"
Perception Disturbance: denied
Behavioral Disturbances: poor impulse control
Attitude towards the Examiner: uncooperative, verbally aggressive, and augmentative
Suicidality/Homicidiality: Denied
Cognition: Alert & Oriented X4 (name, place, day & situation)
Memory: Unimpaired
Judgment/Insight: impaired
Assessment:
Severe mood disorder with psychotic features (disorder)
(F31.64/296.64) Bipolar disorder, current episode mixed, severe, with
psychotic features modified 6 Jan, 2020
Schizoaffective disorder, bipolar type (disorder) (F25.0/295.70) Schizoaffective disorder, bipolar type modified 6 Jan, 2020
Plan: Patient Instructions/Plan
recommended psychotherapy
Medication(s):
Start these medications below:
Refused to restart Risperdal and Depakote and wants to be restarted on Vraylar and Lamotrigine
Declined to sign the med. consent form and mother stated that patient can sign
-Patient informed that dose may be titrated as needed to targeted symptoms relief
-Discussed medication education/risks/benefits/adverse side effects/black box warning in details with patient & mother
-Patient and mother consented to proposed treatment plan with the above medication(s)
Psychoeducation:
-Brief supportive counseling, validation, and supports provided
-Provided education regarding diagnosis, treatment plan, and importance of psychotherapy
-Reviewed medication indications, use, need for adherence to prescribed medication, handling, and storage.
-Balanced nutrition/hydration/participation in physical activity encouraged
-Provided education on sleep hygiene
Safety Plan:
-reviewed safety plan with patient
-ER precaution and/or to call 911 or PMHNP if there are any safety concerns
-mother agrees to monitor for safety and support safety plan
-advised to seek services with the nearest crisis in the event of harm to self or to others
CURES:
Reviewed (1/04/2022)
No concurrent usage of legal/formal high-risk medication(s)
Return-to-Clinic: 2 weeks or sooner if needed
|
CC: Bipolar Disorder.
Psych Symptom/Follow Up:
54 year old LGBT Caucasian male with Bipolar Disorder & HIV,
says he is upset as his car was stolen yesterday but recovered in the
evening, thinks it is a part of the gangstalking that he has been
complaining about for a while, feels he is still being gang-stalked,
otherwise appears calmer, sleeping well, thinking is more organized,
Vraylar has had positive response, Has stopped taking Ativan.
no intention of hurting self or others,
He does not own a gun,
ROS: Overweight
Photosensitivity
HTN
DM
Medications: Vraylar, 1 cap(s) orally at every bedtime (Edited by MUBASHIR FAROOQI on Jan 6, 2020)
lamoTRIgine, 1 tab(s) orally 2 times a day (Edited by MUBASHIR FAROOQI on Jan 6, 2020)
MSE: Physically the patient appeared disheveled. Emotionally the
patient appeared angry and anxious. Attitude in the interview consisted
of cooperation. Observed behaviours included psychomotor agitation. The
patient presented with speech that was normal in rate, rhythm and
articulation. Mood was ambivalent and his affect was anxious. The
patient's thought process was normal and his thought content consisted
of guilty ruminations and obsessions.
Assessment:
Severe mood disorder with psychotic features (disorder)
(F31.64/296.64) Bipolar disorder, current episode mixed, severe, with
psychotic features modified 6 Jan, 2020
Plan:
Lamotrigine 200 mg BID, Vraylar 6 mg po qd.
RTC 8 weeks.
|
| Health Care Providers |
| NI |
|
Julitza Reyes
|
1809 W Redlands Blvd
Redlands, CA 92373-8054
Address
|
|
|
|
Document Details
Inland Psychiatric Medical Group
1809 W Redlands Blvd
Redlands, CA 92373-8054
Address
May 14, 2022 : -
Julitza Reyes
Published
| Powered by
Kareo Clinical
|
----------------------------------------------------------- I REQUIRE A COMMUNITY-LEVEL APOLOGY! INCLUDING THE POLICE DEPARTMENT!
----------------------------------------------------------
When and How to Cut the Ties of Bad Family RelationshipsI'm passionate about health, wellness, social issues and relationships. I offer relatable content and solid advice. What Is Family?In
just a few words...family defines us. Our first relationships were our
family relationships. It's a significant part of who we are to the core,
because our past is an integral part of how we view ourselves and the
world. An interesting aspect about families is that people can
tolerate more bad than good, and even a strained family relationship can
be considered satisfying. ‘My family drives me nuts, but I love them’. Families
can simultaneously be the ones to cause you distress, but are also
there by your side in tough spots. That's a fair trade: Take the good
with the bad. It’s when the bad outweighs the good, or the bad is abuse, that we have to evaluate the health of that relationship for our own wellbeing.
Unconditional
love is the key ingredient in a healthy relationship; one of acceptance
and expression, the ability to agree to disagree at times, and mutual
respect without having to change or control each other. These are ideal conditions though, and for some, it's never been this way with certain family members. These
unbalanced relationships are the worst to endure because family means
so much to us personally and within our culture/society. Unfortunately,
many people are faced with the excruciating decision of whether or not
to continue an unhealthy family relationship with a parent, sibling,
grandparent, son, daughter, or step-family members. If you feel
that you have to cut ties, it's usually because you've endured years of
discontent (or even abuse) and you have no other choice. Many who are
reading this have endured too long.
Just because someone shares some DNA with you they get to take your
stuff? Call you names? Demean you? Sabotage your relationships and
career? No way!
— Dr. Phil McGraw
Evaluating the RelationshipChances
are you've been evaluating the strained relationship for a while, but
committing to cutting the ties brings on feelings of guilt, failure,
shame, emptiness, doubt, abandonment, and even grief. Deciding to face these feelings and manage them is a brave step. No
matter how strained, intolerable, and/or abusive the relationship is,
it's a difficult decision to make. Asking yourself the questions below
can help.
- What's the history? Psychologists
have an old saying: "The best prediction of future behavior is past
behavior." Having extensive history is what hurts the most when breaking
up with a family member, but if that history has been chronically
negative, this can make it easier to make an informed and intuitive
decision. It will be hard to let go of the relationship or put some
distance between you if there were good times along with the bad. It can
still be difficult to cut ties if it's been a long, torturous road.
Even familiar abuse and patterns are hard to break away from. Sometimes
it helps to put it all on paper— one column for positives and one for
negatives—so that you can see both sides objectively. Or give a point
system to each good thing and each bad thing. Sometimes a really bad
thing is much worse than 10 good things. Watch out for patterns that
show the relationship is getting progressively worse. Also, if they keep
insisting they've changed, then keep your eyes open to determine if
their actions show that is indeed true. Even if they have changed, the
relationship dynamic can remain the same.
- Who else is affected by this relationship?
Sometimes, breaking ties with one person means you could have the entire
family upset with you. Remember, other family members have likely
contributed to the abusive person's tactics as well. They may not be
prepared to face that- you are disrupting family patterns. Be prepared
and know that not everyone will understand your decision. It's important
to find a way to manage other family relationships and evaluate the
effects on others as well, but you are not responsible for everyone's
feelings. Don't hesitate to cut ties if the only reason you are keeping
contact is to please the "family" or someone else in the family. Group
enabling is sad but common within families.
- Consider the kids. If you have children, explain in
age-appropriate language to your kids why they may not see their
grandma or aunt for a while. Kids tend to get caught in the middle— some
family members use them as pawns so be as honest as you can with them,
considering they often know more than they let on.
- How is the stress affecting your personal life and current family?
Many people get confused and think their parents or the family they
were born into is more important than the family they build for
themselves. This is wrong. Your original family should never get between
you and your current family. Your wife/husband and kids now take
precedence over your mom and/or dad, so don't tolerate original family
members if they negatively affect your current family. Preferably you,
rather than your spouse, should handle your own family members.
- What's your role? We take on a label or role from
an early age in the family unit. Sometimes we get stuck in that role and
transfer it into our lives beyond the family. Breaking this role and
its effect on our lives may require distance or cutting ties to make a
clean break and change our habits, not only within the family, but in
our current relationships. Your role in the family could be "the baby”,
the “troubled one”, “shy one”, “the black sheep”. Or you might be "the
fixer“ and “mediator” - one who keeps the peace at all costs, taking
care of everyone else. Sometimes a family needs a “scapegoat”, one to
blame everything on. Those willing to speak up, or the squeaky wheel,
are usually the people who are ostracized and shamed. Don’t let the
family problems fall on your back. Do the roles you have in your current
relationships (work and personal) resemble roles you play in your
family?
- How do they feel about you? The best indication of
how another person perceived us is how we feel when we’re in their
presence— more specifically, how we feel about ourselves in their
presence. I know that I feel small, invisible, and out of control when
around a certain family member. I realize that’s how they likely view
me, either on a conscious or subconscious level. Ideally, family should
be based on unconditional love. If you're not feeling the love, then
what are you feeling? Sometimes it's helpful to ask yourself when was
the last time you felt loved by that person, without strings attached.
If you feel awful when that person is around, it's probably triggered by
their ugly feelings about you. Picking up on subtle cues may help you
realize the truth of that relationship. In other words, the feeling may
be mutual, they just may show it in passive-aggressive ways. Keeping
that in mind, remember that it's not your fault they feel this way.
- Are there any boundaries? One thing many families
have in common is a lack of boundaries: People say what they want, do
what they want, and respect is nowhere in sight. That can work for some.
However, it's unhealthy to equate a lack of boundaries with
unconditional love. Specialists agree that for children, having
boundaries gives a sense of being loved, and childhood is where some of
the mayhem started between family members. If you're still undecided
about cutting off the relationship, setting healthy boundaries now can
show you where you stand. Although, it is more difficult to set
boundaries with family than with any other people because patterns are
ingrained for generations sometimes. As a child, you quickly realize
adults set not only the rules, but the boundaries (or lack of) as well.
We were often taught unhealthy boundaries from the people we needed them
with. When the child becomes an adult, they are able to set their own
boundaries.
- How close are you? Often, moving away symbolizes a
new life away from our family. It can ease tension by being located
cities or states away! If the person you have problems with lives far
away or you don't see them often, you can tolerate them only
periodically and carry on with life as usual. A quick visit with the
negativity and drama — maybe two holidays each year— might be
manageable. If it causes too much pain and drama, keeping in touch (even
through emails) may not be worth the hurt and pain.
- Is resolution possible? Some
families refuse to speak about issues at all. Perhaps the same issues
come up repeatedly then a possible resolution may be a big, fat NO.
Sometimes the answer is "no" right now, but can change later down the
road. Don't bother hashing out major issues between the person and
yourself— you've probably tried this in the past and walked away with a
big heaping serving of that person's denial, hostility, and
self-preservation. As children, we are powerless against family members
because we're too young to have a voice or shamed and guilted if we
express ourselves or our needs. Sometimes that pattern follows us into
adulthood. Remember, any decision can be temporary. If the ties are cut
right now, they may be mended later. Cutting ties isn't always an open
and close, final case.
Read More From WehavekidsOne
more thing: Sometimes, instead of having an issue with one person, the
problem lies with more than one or even an entire branch of the family.
In that case, it's best to evaluate the issues as a whole. It could be
that letting go of an entire chunk of your family is necessary.
Daring to set boundaries is about having the courage to love ourselves, even when we risk disappointing others.
— Brene Brown
It's Okay to Say Goodbye When...- The
relationship is physically or mentally abusive. Don't downplay the
effects of these kinds of abuse, especially long-term. It may take
counseling to realize you've been abused. We may think of abuse as
"this" or "that", but there are many grey areas where abuse is defined
by us personally. Just as trauma doesn't have to be something BIG, it is
something that we're personally unable to manage.
- It causes enough stress that it affects important aspects/areas of your life, like work or home life.
- You find yourself spending a lot of time thinking about, ruminating
about the sour relationship, and losing sleep over it. Don't
underestimate how lack of sleep and stress affect your health.
- The relationship is one-sided when there is no valid reason why there isn't some effort made by the other person.
- Patterns repeat themselves. You set boundaries for instance, and the
other person respects them for a couple of weeks then completely
disregards them or they keep coming back to ask for money or do them
favors. It is their way to confuse and use emotional tactics to keep you
"hooked".
- The relationship is only about borrowing money or bailing them out
of trouble. Don't get dragged down with them or involved in risky
business and legal trouble, even if they are family.
- The person is using gossip to manipulate and control you and/or other family members against you.
- All contact with them is negative. They only call to bring you down
and put you down, too. They focus on their problems without concern for
your time or how you are doing.
- There are negative consequences every time this family member
doesn't get what they want from you. They find ways to punish you if you
don't play their way.
- They play childish games— the silent treatment, blame games— and there is no talking to them. It's their way or no way.
Most people know intuitively when it's time to cut ties. Listen to yourself.
Cutting people out of your life doesn't mean you hate them, it simply means you respect yourself. Not everyone is meant to stay.
When You Decide to Sever Ties with a Family Member...- Try it out... less contact
through calls, visits, and emails. This is especially important when
the relationship represents emotional ties. Breaking the pattern of
mental/psychological abuse helps to shed light on how the person affects
you so you can make clear-minded decisions. In therapy, I ask clients
if they could give themselves 6 months off from the relationship. This
is often enough time to gain a better perspective.
- Heal yourself first. Sometimes working on ourselves
and boundaries with others in our current relationships has a domino
effect and can help give us the confidence to do the same within family
relationships. Cutting ties for the sake of healing yourself is a worthy
cause too. Instead of focusing on the other person, focus on your
healing and you'll get much further in your personal journey and healing
than you can imagine.
- Set a few boundaries/skip a holiday. Sometimes it's
not necessary to cut ties, just adjust them. Even giving a few
ultimatums is okay. Check in with yourself; how you feel before you
decide to go to a family event or see the family member. If your body is
tense and you feel awful, respect that. It's often about listening to
ourselves. Try skipping a holiday, not taking calls from the person if
you don't want to. Minimize the feeling of obligation to them.
- Keep a neutral position. If certain subjects always
end in an argument, avoid them and keep the conversation neutral. If a
family member insists you agree with them or insults you when you don't,
keep your distance.
- Limit contact to times when something major happens.
Send an email to let the family member know you are pregnant, someone
died, you got a great new job, or you're moving to another state. You
might consider including them on family group emails but avoiding
one-to-one exchanges. Keep the messages and announcements positive.
- Know that it's difficult. Death is final, but
cutting ties is like death without the closure. Give yourself the love
and time to grieve because cutting ties is a grief process. You will
probably feel the worst when the first birthday or holiday rolls around,
but you can prepare yourself by practicing self-care rituals as well as
journaling. Remember that these unpleasant feelings are less harmful
than if you had kept the relationship intact. Feelings like guilt and
shame are part of the problem, and they are finally unraveling
themselves and slowly being released. Many feelings you may experience
were the way in which family-controlled you. They must be released to
heal.
- Focus on who you have and who you are. Having a
good support system of friends or other family members makes cutting
ties easier. Maintaining your values is a part of who you are. Knowing
who you are, what you stand for, and who supports you is your North
Star, your compass.
- Don't pretend everything is okay. Don’t minimize
your thoughts and feelings by pretending everything is ok. Pretending
and avoidance are common in dysfunctional families. Speak up!
.png) This
content is accurate and true to the best of the author’s knowledge and
is not meant to substitute for formal and individualized advice from a
qualified professional.
[ I HAVE ABSOLUTELY NOWHERE GO -- NO SOCIAL SERVICES SUPPORT NETWORK ]
I MUST WALK INTO THE STREETS OF HOMELESS AND GO DIE!
NOT A SINGLE PERSON OF SOCIAL CIVIL SOCIETY WILL ADHERE TO REASON!
.gif)
------------------------------
It is now 11:56 PM : I was leaving voice mails the contact numbers listed on:
http://auditor.ca.gov/contactus
Accessibility Contact:
(916) 445-0255
Information Security Officer:
Jeremy Evans (916) 445-0255 x440
Information Privacy Officer:
Chris Dawson (916) 445-0255 x324
Press Contact
(916) 445-0255
Legistative Contact:
Paul Navarro (916) 445-0255
etc....
I have had to dial 911 voice to report that my NEPHEW KICKED IN MY BEDROOM DOOR VIOLENTLY. All I was doing was telling him to get away go away leave me alone. And I started banging with my fist against the inside of the door to tell him o go away. My action was not violent but to cause a sound that would be a higher db level than his need to berate me. to bully me, to command me any other thing than just leave me alone. They won't. They are my mother and him and anything I do is in their need of peacebuilding they won't oblige their obligation and responsibility. Something wrong with this house.
My nephew David was upset because I woke him up attempting to get my mother's healthcare properly prioritized in view of her interrupting what I was doing in this hour.
The 911 voice call is to the San Bernardino Police Department. I was not expecting that to be the outcome of this.
My mother was screaming in agony. She has had some kind of injury over the course of some kind of 2 months or so. I can hear here in agony many nights and many times when I am here attempting to resolve the matters at hand.
I told her at least a month ago that he needed to call the doctor to get some stronger pain medication. She dismisses --- it's ok -- like dismissing the level of her outburst is not to the level of her pain. Whatever that is.
I mentioned that the pain medication she should get is Tylenol with Codeine. You see, even though I do not have an actual license in massage therapy, I did go to school for such at the San Francisco School of Massage.
So, my mother has been psychologically invalidating me for my entire adult life. I do not believe that this was a part of my childhood. It was only when I came out to her as gay did I noticed this for sure a part of my relationship with my mother. I am now 56.
Tonight, she finally actually has the pain medication prescribed but instead of taking it, she is screaming "ah ah it hurt it hurts" so loud I went into her room and again stressed that she needs some pain medication. No human being would allow another human being to suffer like that. She carrying on like pain 10!
The Police Arrived -- San Bernardino Police Officer Beltran
This matter ultimately was stopped at a civil level involvement.
Although the motives of my nephew to bust in the door were violent -- and must conclude he needed to physically assault me. The actions of violence are theirs - not mine.
The same as ending with this 911 text interface and the SMS conversation history with my mother.
Seriously -- HOW FUCKED UP IN THIS FAMILY ARE YOU GOING TO BE TO ME?
911-05-11-2022.vzm
http://fuckeduphuman.space/911-Text-Interface/911-05-11-2022.vzm
----
http://realityaudit.life/Medical-Mental-Health-LawMatters-StandardsOfCare/Family-Driskill/Veronica-Ann-Warnick-Driskill/
Index of /Medical-Mental-Health-LawMatters-StandardsOfCare/Family-Driskill/Veronica-Ann-Warnick-Driskill
Icon Name Last modified Size Description[PARENTDIR] Parent Directory -
[DIR] 9094747652-Mama-FireDancer-05-11-2022-parts/ 2022-05-11 06:38 -
[ ] 9094747652-Mama-FireDancer-05-11-2022 [ Spoken Voice Narrative of Text Conversation].ogg 2022-05-11 09:00 11M
[ ] 9094747652-Mama-FireDancer-05-11-2022.vzm 2022-05-11 06:38 60K
FOR MY ACTIONS? THERE IS NOTHING VIOLENT ABOUT POUNDING ON THE INSIDE OF THE DOOR TO GET ANYONE WHO IS ON THE OTHER SIDE TO STOP AND LEAVE ME ALONE!
I DID NOTHING WRONG!
YOU ALL CAN'T SEE THAT
MY MOTHER WAS JUST PLAYING GAMES EARLIER -- I DON'T BELIEVE SHE IS IN THAT KIND OF PAIN -- SHE IS DOING THIS TO BE A MENTAL CASE ON TOP OF ALL OF THIS!
Going back to leaving voice mails
I was at Legislative Contact
Paul Navarro (916) 445-0255 [ No Extension ]
This message will be referenced as --- VIOLENT INTERRUPTION ---
-----
YOU SEE -- AN WITH AN AUDIT FOR CHANGE WITH SAN BERNARDINO POLICE DEPARTMENT
THEY CONTINUE TO VIOLATE RULES AND LAW WITH IMPUNITY!
WHAT EXACTLY IS WRONG WITH THIS TWEET THREAD?
BUT NOW AT LEAST! WITH AN OFFICIAL GOVERNMENT OFFICIAL POLICY CHANGING THEIR PLACEMENT IN VIEW OF THIS --- NO CHANGE ANYWAY!
Peace Officers—Hate Group Affiliations
Law Enforcement Departments Have Not Adequately Guarded Against Biased Conduct
AUDITOR: "They have not implemented robust community engagement strategies or employee training practices."
NOR AS IT IS - WILL THEY EVER!
adjective adjective: robust; comparative adjective: robuster; superlative adjective: robustest 1. strong and healthy; vigorous. "the Caplans are a robust, healthy lot"
(of an object) sturdy in construction.
(of a process, system, organization, etc.) able to withstand or overcome adverse conditions. "California's robust property market" uncompromising and forceful. "he took quite a robust view of my case"
2. (of wine or food) strong and rich in flavor or smell. "a robust mixture of fish, onions, capers and tomatoes"
Origin mid 16th century: from Latin robustus ‘firm and hard’, from robus, earlier form of robur ‘oak, strength’. Use over time for: robust
MY DEMAND TO HAVE A VIABLE CONVERSATION? WOULD THAT QUALIFY?
AUDITOR: They also stress honoring that commitment by incorporating strategies
for addressing bias into key processes, including recruitment, hiring,
training, community engagement, and misconduct investigations.
THIS CAN NOT CONTINUE!
Auditor:
An additional problem with the local departments' investigations of
biased conduct is that they relied heavily on the officers' denials that
bias influenced their actions, without considering whether an officer's
conduct created the reasonable appearance of bias. This approach is
problematic both because officers are unlikely to admit that bias
affected their actions and because it fails to consider the likely
perspective of the community. We did not find this problem at San
Bernardino Police because the records we reviewed included no evidence
that the department had directly questioned the related officers about
whether their conduct had been motivated by bias.
HOW ABOUT QUESTIONING THE OFFICERS THAT I HAVE PERSONALLY DEALT WITH.
Auditor: The work officers perform is both critically important to our State and
often extremely challenging. We found no evidence that the majority of
the officers we reviewed had engaged in biased conduct. Nonetheless,
biased conduct by even a few officers can cause harm to members of the
public and erode the community's trust in law enforcement. For these
reasons, it is incumbent upon law enforcement departments and the State
to take the steps necessary to guard against officer bias in all its
forms.
SOUNDS LIKE A NEED FOR SUPERMAN -- BECAUSE NO OTHER PROTECTIVE ACCOUNTABILITY AGENCY IS AVAILABLE!
---
Phone:
(916) 445-0255
Address:
621 Capitol Mall, Suite 1200
Sacramento, California 95814
Whistleblower Hotline:
Call (800) 952-5665
Fax (916) 322-2603
File a complaint online
Legislative Contact:
Paul Navarro | (916) 445-0255
Press Contact:
(916) 445-0255
Information Privacy Officer:
Chris Dawson | (916) 445-0255 x324
Information Security Officer:
Jeremy Evans | (916) 445-0255 x440
Accessibility Contact:
(916) 445-0255
I received this from my mother:
-----
SO EXACTLY WHAT HAPPENED? A VIOLATION OF THE 1ST AMENDMENT!
ABSOLUTELY NO CHANGE! EXACTLY WHAT IS WRONG WITH MY TWEETS? OH THEY REPRESENT THE TRUTH!
EVEN AFTER THEIR AUDIT!
==========================
The 3d Model on right is called "Crackdown Agent Female"
Mama, you are still just playing games.
Wanting me to help you last night!
ABSOLUTELY NO!
TRY GOING TO:
-----------------
--------
Kareo Patient PortalMessages
[ Keeping it Real ] -- There is an emoji for this [ 💯]
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 4:47 PM
The meaning of that emoji is a SCORE of 100% or of EXCELLENCE!
I had not logged in for a while to Inland Psyche / Patient Portal because none of my records were updated and the interactions with my doctors are as I have said they are. I am the patient and the patient has had something to say profoundly to the criticism of what has been the operating agenda of this entire equation seems way offensive off the mark offensive.
I write about it online and have given it a tag [ #BigManKillingTechBug ]
I do not accept that you all just turn around [ for me ] and that turnaround does not apply to real true grit policy and change in your organization. I do not accept an underhanded change that now puts items into my medical record. Especially considering I have not even checked it for errors and/or omissions. I NEED TO HAVE A DETAILED LOG OF WHEN THE DETAIL WAS UPDATED TO MY RECORDS!
WITHOUT DECEPTION! This whole thing has shattered my family relations!
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 5:05 PM
THIS IS A GRAPHIC THAT SHOWS A VERY TRUTH!
THE QR CODE IN THAT GRAPHIC IS:
http://realityaudit.life/ShortURLS/DasdardlyAgainstTheUSA/08/
I SUGGEST THAT YOU LINK TO IT - FOLLOW THE DIRECTIONS ON THE ORDER TO HOW TO RECEIVE THAT PAGE.
NOTE THE LENGTH OF THE PAGE -- IN THE AUDIO THERE IS DIRECTIONS -- FOLLOW THAT DIRECTION.
YOU MAY TAB TO THE END OF THE PAGE TO REFLECT THIS FOOTNOTE: [ Next Message ]
.png)
- -----[ SOURCE ASSOCATION TO REALITYAUDIT ]-----------[ Not Provided On Kareo ]------------
OF SPECIAL IMPORTANCE:
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 5:06 PM
-------
FROM ALL SIDES -- GOD IS HERE!
IS THAT NOT THE QUEEREST THING YOU EVER HEARD?
JamesMartinDriskill-BornSeptember1st1965DiedNotSureHomeTownSanBernardinoCaliforniaUnitedStatesofAmericaTheEarthSolarSystemSolMilkyWayGalaxyTheUniverse!
ThisIsNotTheWayToTreatASingleHumanBeing!
HumanityHasCompletelyLostItsPurposeToBeHere!
GoodBye!IDied!Free!
KnowingTheTruthIsTheTruth!
ThisTruthIsTheReal! TheTruthTheWholeTruthAndNothingButhTheTruthTheRealTruthTheRealUpTruthTheRealUpHumanTruthTheAbsoluteRealUpHumanTruthTheAbsoluteRealUpHumanMoralTruth!
TheyWillNotHaveMercyOnYourSouls!
TheyWillNotHaveMercyOnYourSouls!
TheyWillNotHaveMercyOnYourSouls!
Mama-ICryandScreamToTheHighestLoudestHighestLoudestVolumeICanMusterOutOfMyVoice!
Mama-StilYouWantToFight!
Mama-YouWillNotStopAtAnyKindOfCallinOut!
------
[ continued]
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 5:07 PM
Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy![22]
Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy![44]
Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy![66]
Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy! Mercy![88]
NothingHereTo - Cell - A - Barate!
Mama-HowCanYouBeSoCruel?
Mama-This Unforgivable!
Mama-YouAreFireDancer!
Mama-YouDeserveYourDestinyWithFlames!
Mama-BurnBurnBurnInHell!
------
Seriously Doctors, You are the fault of shattering my family relations.
-
James Driskill
i tried to send this already -- I had an error.,
-
James Driskill
I have a PUBLIC UPDATE to the EMAIL that includes a
copy of this messaging,
includes in full a copy of my medical record
includes my interactions with communication with
https://ncd.gov/ - I attended and provided chat input
to their council meeting on May 11th 2022.
PROFOUND STATEMENTS I HAVE WRITTEN
Includes my description of why 911 was called last night
after my bedroom door was kicked in by my nephew
David Allen Driskill when he would not leave leave me alone.
Officers were dispatched to the house.
Include my interactions with Auditor.ca.gov,
in relation to:
http://auditor.ca.gov/reports/2021-105/index.html
Term [ San Bernardino ] is mentioned 76 times.
Also mentioned in this public update is this:
When and How to Cut the Ties of Bad Family Relationships
L Izett
Mar 8, 2022
SERIOUSLY DOCTOR -- YOUR SCHEME OF SILENCE HAS SHATTERED MY FAMILY RELATIONS!
Someone in all true honesty needs to step up and help fix this -- IMMEDIATELY!
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 6:04 PM
Tone detector
BETA
How this may sound to readers:
💡inspirational
🙂joyful
🤝confident
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 6:08 PM
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 6:09 PM
My Mother has directives to listen to this audio as well. Once we all have the issues prioritized, then we can proceed with the REALITY AUDIT in all truthfulness -- and bring forward the correct interface here,.
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 6:09 PM
This COMMUNICATIONS requires a REPLY
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 7:04 PM
Some corrections
Which does have pointers outside of our informational society that goes to show that the record was just thrown together.
The first thing, you might want to understand is trust. The lack of trust involved in all of this is real, not imaginary.
"Irrelevant details" is what you call my first encounter with "CHINYERE OBAKHUME" ?
THE SAFETY PLAN IS COMPLETELY ILLOGICAL -- CONSIDERING THE RECORD HERE:
http://fuckeduphuman.space/911-Text-Interface/ [ That is a REALITY ]
-- 911 is not available for persons who are TARGETED INDIVIDUALS!
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 7:11 PM
https://www.goodreads.com/book/show/43826597-the-governors-of-gangstalking
"I & A Office coordinates between the Fusion Centers and works with the Emergency 911 Call Centers in the United States, to block and redirect the emergency calls of Targeted Individuals. Many Targeted Individuals have experienced what happens "
---
This statement in the public genre of the gangstalking element of life, is shown with evidence proven by both 911-text-interface as well 911 call recordings documented. This has been my main complaint, as a TARGETED INDIVIDUAL without the ability to address this issue, this SERIOUSLY EFFECTS the chart of "SAFETY NEEDS" under the Maslows Hierarchy of Human Needs. There is no SAFETY NEEDS met. THAT IS THE ISSUE THAT MUST BE BROUGHT INTO MENTAL HEALTH AWARENESS AND TREATMENT.
There are other corrections that need to be assessed in this medical record. You will note, that this Kareo conversation is added to the end of the audio text.
-
James Driskill
to JAGAN MOHAN RAO JAKKULA
5/14/22 7:11 PM
Tone detector
How this may sound to readers:
💡inspirational
🤗friendly
☝️assertive
| 11 attachments |  | | 1652595419482.png
189K |
| ) | | 1652595419436.png
181K |
| ) | | 1652595419575.png
442K |
| ) | | 1652595419761.png
588K |
| ) | | 1652595419466.png
179K |
| ) | | 1652595419563.png
244K |
| ) | | 1652595423045.png
6529K |
| ) | | 1652595419230.png
36K |
| ) | | 1652595420709.png
1962K |
| ) | | 1652595420742.png
1962K |
| ) | | image.gif
1K |
|
|
|




 1 and
1 and 


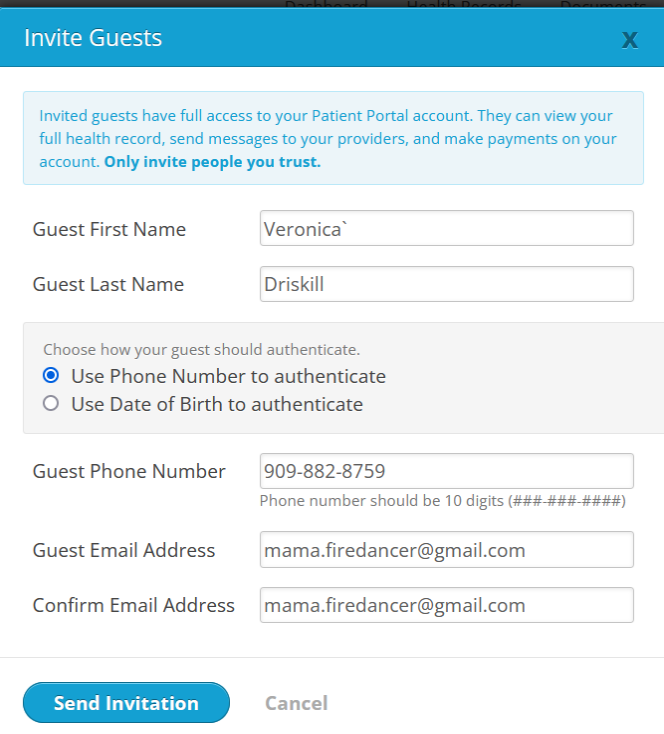




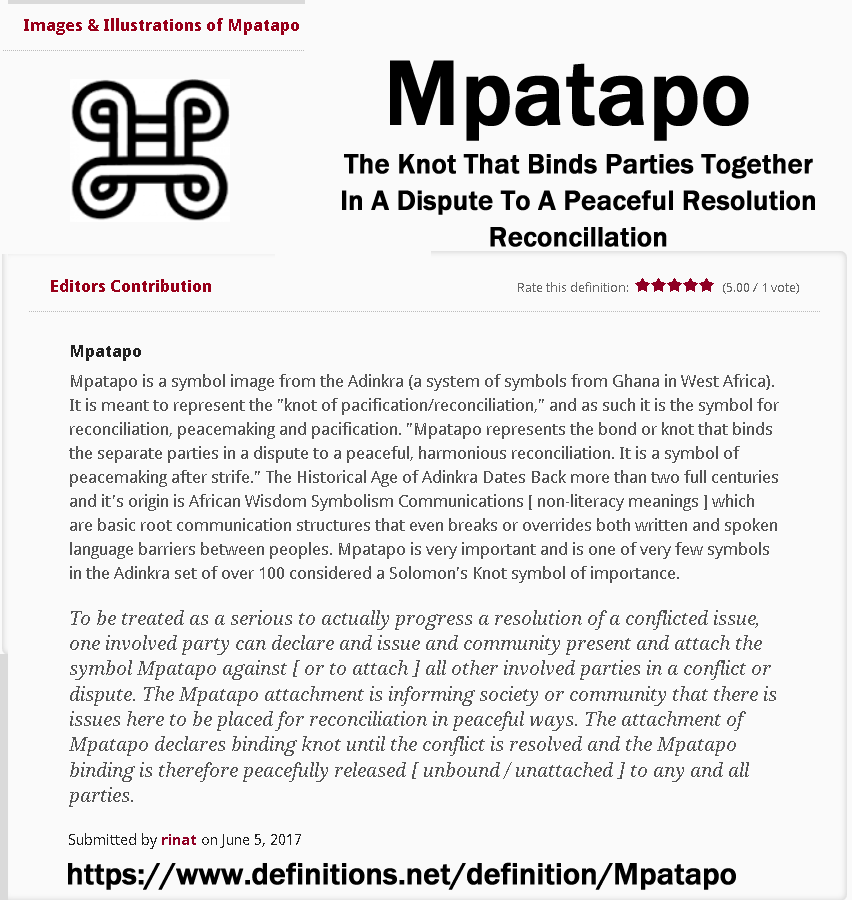

.png)
.png)
.png)
.gif)
![[PARENTDIR]](./Gmail - Fwd Family Matters Really This family sucks!_files/unnamed(6).gif)
![[ ]](./Gmail - Fwd Family Matters Really This family sucks!_files/unnamed(7).gif)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.jpg)
.png)
.jpg)
.jpg)
.jpg)
.jpg)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
![[TXT]](./Gmail - Fwd Family Matters Really This family sucks!_files/unnamed(42).gif)
![[DIR]](./Gmail - Fwd Family Matters Really This family sucks!_files/unnamed(43).gif)
![[IMG]](./Gmail - Fwd Family Matters Really This family sucks!_files/unnamed(44).gif)